Azahp Form
Azahp Form - This new feature can be used to complete the azahp practitioner data form for contracted providers submitting. Please complete each section leaving no blank spaces. Healthcare providers that want to serve patients in the arizona health care cost containment system (ahcccs) must join a health plan,. Web based on the recommendations and approval from the arizona alliance of health plans (azahp) credentialing alliance, the following forms have been updated:. Copy of your clia certificate (if applicable) please fax completed application with all required documents to. For newly contracted providers, please email forms to azchpotentialprovider@azcompletehealth.com.
Simply click on one of the forms below and follow the. Web this form includes personally identifiable information (pii) such as practitioner name, date of birth and ssn and should be sent in a secure manner. Non delegated group azahp roster. Web this form includes personally identifiable information (pii) such as practitioner name, date of birth and ssn and should be sent in a secure manner. For newly contracted providers, please email forms to azchpotentialprovider@azcompletehealth.com.
Fill Free fillable Directions for completing the AzAHP Practitioner

Web this form includes personally identifiable information (pii) such as practitioner name, date of birth and ssn and should be sent in a secure manner. Web about the azahp credentialing alliance. This new feature can be used to complete the azahp practitioner data form for contracted providers submitting. Directions for completing the azahp practitioner data form (azahp) 1. Becoming a.
Azahp Form Complete with ease airSlate SignNow

Arizona department of child safety. Non delegated group azahp roster. For newly contracted providers, please email forms to azchpotentialprovider@azcompletehealth.com. Web this form includes personally identifiable information (pii) such as practitioner name, date of birth and ssn and should be sent in a secure manner. For existing network providers, please.
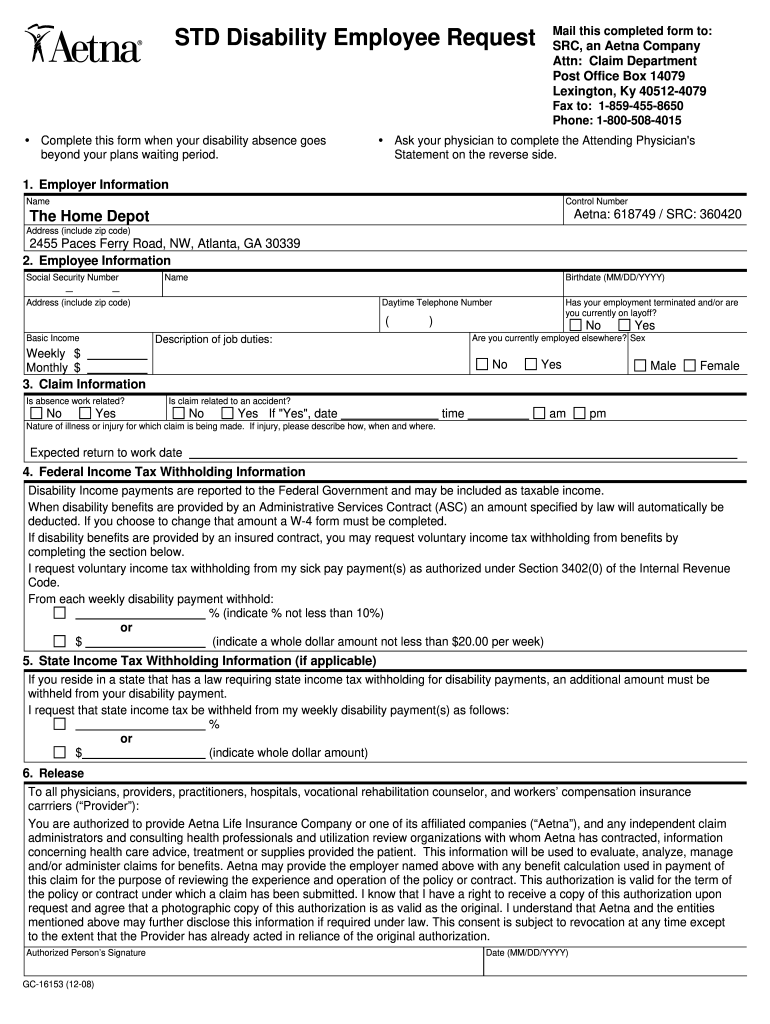
Fillable Online Short Term Disability Claim Form Fax Email Print A20
Web this form includes personally identifiable information (pii) such as practitioner name, date of birth and ssn and should be sent in a secure manner. Copy of your clia certificate (if applicable) please fax completed application with all required documents to. Web submit a provider interest form and attach the required azahp forms (located below). Web this form includes personally.
AZPDES Form 2D Fill Out, Sign Online and Download Printable PDF

Non delegated group azahp roster. Web azahp practitioner data form directions for completing the azahp practitioner data form (azahp). Web facility credentialing & recredentialing application. Any questions regarding this form, please check with your health. Arizona department of child safety.
Fillable Online AzAHP Organizational Data Form Health Choice Arizona

Clearly state if information requested is not. For newly contracted providers, please email forms to azchpotentialprovider@azcompletehealth.com. Web how to become a provider of bcbsaz health choice. Web azahp practitioner data form. Web facility credentialing and recredentialing application instructions.
Azahp Form - Any questions regarding this form, please check with your health. Directions for completing the azahp practitioner data form (azahp) 1. Web this form includes personally identifiable information (pii) such as practitioner name, date of birth and ssn and should be sent in a secure manner. Web this form includes personally identifiable information (pii) such as practitioner name, date of birth and ssn and should be sent in a secure manner. For newly contracted providers, please email forms to azchpotentialprovider@azcompletehealth.com. Web this form includes personally identifiable information (pii) such as practitioner name, date of birth and ssn and should be sent in a secure manner.
Web the arizona association of health plans (azahp) is pleased to announce the creation of a new credentialing alliance aimed at making the credentialing and recredentialing. Web facility credentialing & recredentialing application. For newly contracted providers, please email forms to azchpotentialprovider@azcompletehealth.com. Any questions regarding this form, please check with your health. Please complete each section leaving no blank spaces.
Web How To Become A Provider Of Bcbsaz Health Choice.
Becoming a contracted provider with bcbsaz health choice is easy! Web about the azahp credentialing alliance. Web azahp practitioner data form directions for completing the azahp practitioner data form (azahp). Any questions regarding this form, please check with your health.
Healthcare Providers That Want To Serve Patients In The Arizona Health Care Cost Containment System (Ahcccs) Must Join A Health Plan,.
Web based on the recommendations and approval from the arizona alliance of health plans (azahp) credentialing alliance, the following forms have been updated:. Web this form includes personally identifiable information (pii) such as practitioner name, date of birth and ssn and should be sent in a secure manner. Please complete each section leaving no blank spaces. Simply click on one of the forms below and follow the.
Click To Report Child Abuse Or Neglect.
Web facility credentialing and recredentialing application instructions. Directions for completing the azahp practitioner data form (azahp) 1. Web this form includes personally identifiable information (pii) such as practitioner name, date of birth and ssn and should be sent in a secure manner. Banner health network | provider interest form.
Clearly State If Information Requested Is Not.
Web this form includes personally identifiable information (pii) such as practitioner name, date of birth and ssn and should be sent in a secure manner. Web the arizona association of health plans (azahp) is pleased to announce the creation of a new credentialing alliance aimed at making the credentialing and recredentialing. Web submit a provider interest form and attach the required azahp forms (located below). Web facility credentialing & recredentialing application.